By Calli | Licensed Chiropractor & Esthetician | May 3, 2026
You stand up from your chair and there it is — a sharp, almost electrical pinch in the front of your hip. You stretch. It eases for a minute. You sit back down. It comes right back. By the end of the day, the front of your hip feels bruised from the inside out.
If that’s you, you are not imagining it and you are not just tight. The pinch is a mechanical signal — and once you understand what is actually getting compressed and why, fixing it becomes far simpler than most people think.
Quick Summary
The pinch you feel when sitting is usually anterior hip impingement — soft tissue or the joint capsule getting squeezed at the front of the hip socket. The cause is rarely the hip itself. It is the position of the pelvis, the weakness of the glutes, and the hours your hip is held in deep flexion. This article walks through the mechanism in plain language, the modern habits driving it, a 5-minute reset routine, and the signs that mean it is time to see a clinician.
In This Article
1. Why your hip pinches when you sit
2. The modern posture habits making it worse
WHY TRUST THIS ARTICLE
Written by Calli — a licensed Doctor of Chiropractic (DC) and Licensed Esthetician (LE) practicing in Los Angeles. Every claim here reflects clinical observation from real patient cases, current orthopedic literature, and practice-based protocols. Educational content, not a substitute for a hands-on examination.
1. Why Your Hip Pinches When You Sit
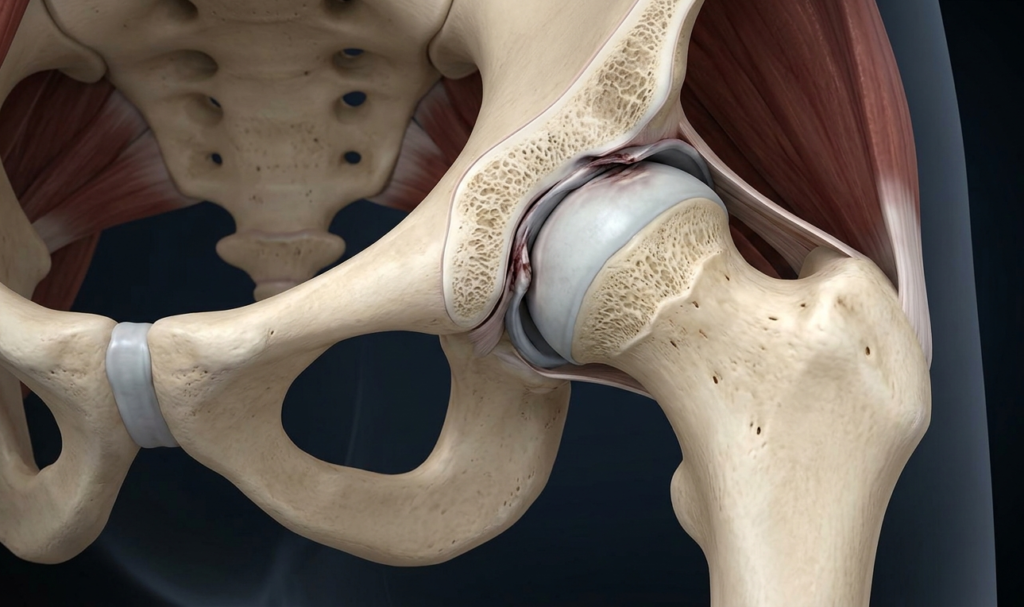
The hip is a deep ball-and-socket joint. When you stand, the head of the femur sits comfortably in the socket and the joint capsule, labrum, and surrounding tendons all have room to move. When you sit — especially in a typical office chair with your knees roughly level with your hips, or a soft couch where your knees rise above them — the femur is driven up and slightly forward into the front rim of the socket. That front rim is where soft tissue gets pinched.
The medical name for the mechanism is anterior femoroacetabular impingement, often shortened to FAI. The pinch you feel is not just tightness and it is not a pulled muscle. It is a real geometric collision — something is being squeezed between two bones every time you go into deep hip flexion.
What the pinch is, and what it is not
Most people describe a sharp, focal pinch in the crease of the hip — the line where the thigh meets the lower abdomen. Some feel it deeper, almost into the groin. It is rarely a burning or shooting pain — that profile points more toward nerve irritation, which is a different problem. A true impingement pinch is mechanical: it shows up at a specific position, eases when you change position, and returns the moment you go back to deep flexion.
It is also not the same thing as a tight hip flexor. People assume the front of the hip feels tight because the muscles are short, but in the office I see far more cases where the muscles are actually overworked because the joint mechanics underneath them are off. Stretching the hip flexor in those cases often makes the pinch worse, not better.
2. The Modern Posture Habits Making It Worse
If hip impingement were purely about anatomy, it would always have been common. It has surged in the last fifteen years for one reason: we sit differently than humans ever have, and we do it for ten to twelve hours a day. I unpack the broader downstream effects in my guide on what sitting all day does to your spine, but for the hip specifically, three habits drive the pinch.
Long, deep, unbroken sitting
The single biggest factor is duration. The hip is designed to load and unload — to move through ranges, take pressure, then release it. When you sit for two or three hours straight, especially with knees high or legs crossed, the front of the joint capsule stays compressed the whole time. Tissue that is starved of normal motion responds the way any tissue does: it stiffens, swells slightly, and the next time you bend forward in your chair to read a screen, that already-irritated tissue gets pinched again.
A pelvis that has forgotten neutral
Most desk workers sit with the pelvis tilted backward — the lower back rounds, the tailbone tucks under, the front of the hip jams forward into the socket. This is a posture the body learns. When someone with a tucked pelvis stands up, they often keep that pattern. The pelvis stays tilted, the hip joint stays in a partial impingement position even when standing, and the front of the hip never gets a real break. Over months and years, this is what turns occasional pinching into chronic pinching.
Glutes that have stopped working
The glutes are the engine that holds the hip joint in proper alignment. When you sit on them all day, they go quiet — the brain stops recruiting them efficiently. Then, when you stand and walk, smaller muscles around the hip flexor try to stabilize a job that was never theirs. They overwork, they irritate the joint capsule, and the front of the hip pays the price. This is why stretching alone almost never solves a chronic pinch — the issue is weakness, not tightness.
3. A 5-Minute Reset You Can Do Anywhere
There is no single stretch that fixes hip impingement. What works is a short sequence that decompresses the joint, restores pelvic neutral, and wakes up the glutes — done often enough that the body relearns the pattern. This is the routine I give patients to use during their workday.
Step 1 — Open the hip (90 seconds)
Stand facing a wall, hand on the wall for balance. Take a long step back with one leg, keeping that back leg straight and the heel pressed into the floor. Square your hips to the wall and tuck your tailbone gently downward. You should feel a stretch through the front of the back hip. Hold for 45 seconds, then switch sides. The goal is not to feel a deep stretch — it is to feel the front of the hip lengthen and the pelvis sit in a more neutral position.
Step 2 — Wake the glutes (90 seconds)
Stand tall with feet hip-width apart. Squeeze your glutes — not just clench, but actively contract — and hold for 5 seconds. Release. Repeat ten times. This sounds laughably simple, but for desk workers whose glutes have been quiet for hours, the act of consciously firing them is what restarts the connection between brain and muscle. Then, holding the squeeze, do ten standing hip extensions per side: keep one leg straight, drive the heel slowly backward without arching your low back, and squeeze hard at the top.
Step 3 — Reset the pelvis (60 seconds)
Stand against a wall — heels, hips, shoulders, and head all touching. Without lifting your heels, gently flatten your low back into the wall by tucking your pelvis very slightly. Hold for 10 seconds, release halfway. Repeat six times. This re-teaches the pelvis what neutral feels like. Once you have practiced it standing, the same control transfers into how you sit.
Done two or three times during the workday, this five-minute routine will outperform an hour of static stretching at night. The reason is simple: the problem is created by sitting, so the solution has to interrupt sitting — repeatedly.
4. When Self-Care Is Not Enough
Most cases of sitting-related hip pinch resolve once posture changes and the glutes start firing again. But not all. There are signals that mean the problem is structural enough to warrant a hands-on assessment, not another stretching protocol.
Signs to take seriously
Persistent pinching that has not improved after three or four weeks of consistent posture work. Pain that wakes you up at night. Clicking, catching, or a sense that the joint is locking. Pain that radiates into the groin or down the thigh. Loss of range — for example, you can no longer comfortably tie your shoes, sit cross-legged, or get into a deep squat. Any of these is a reason to see someone trained to evaluate the joint itself, not just the muscles around it.
What a chiropractor or physical therapist actually does
A first visit usually involves a posture assessment, a series of orthopedic tests to rule out labral or structural issues, and a hands-on evaluation of how your pelvis is moving. Treatment is rarely a single thing. It typically combines joint mobilization to restore proper hip mechanics, soft-tissue work on the surrounding muscles, and a corrective exercise plan that is specific to which part of the chain is failing in your case. If the joint itself is structurally compromised — for example a labral tear or a cam-type bony impingement — we refer out for imaging. The point of the assessment is to know which problem you actually have, so the work you put in matches the cause.
Calli’s Clinical Note
In my office, the patients whose hip pinch resolves fastest are not the ones who stretch the most — they are the ones who change their sitting interval. Standing up every 30 minutes, walking for two minutes, doing one round of glute squeezes, then sitting back down. That single habit, more than any one exercise, is what unloads the joint enough to let it heal. The exercises matter; the rhythm of sitting matters more.
The Bottom Line
A hip that pinches when you sit is almost always a posture and glute problem disguised as a hip problem. Stand up more often, reset your pelvis when you do, wake up your glutes — and most pinching settles within a few weeks. If it does not, or if a red flag shows up, a hands-on evaluation will save you months of guessing.
Related Reading
Shoulder Impingement Syndrome — A Chiropractor Explains — the upper-body version of the same compression mechanism. If you sit at a desk, you often have both.
Hip pinching gets confused with sciatica all the time — but they have completely different mechanisms and different fixes. In the next article I walk through how to tell the two apart and the protocol I use in the clinic.
— Calli
DC, LE | Licensed Chiropractor & Esthetician | Aligning the body, glowing the skin, one habit at a time.
Medical disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Hip pain has many possible causes, including structural conditions that require imaging or specialist care. Always consult a licensed healthcare provider for an evaluation specific to your case.