There is a test I do in the first five minutes of every shoulder evaluation that almost no one in my patients’ prior care history had ever tried. I ask the patient to stand relaxed, arms hanging at their sides, and I look at where their palms face. Not where their arms are — where their palms face.
In rounded shoulders, the palms rotate inward and slightly backward. In anterior humeral glide — the condition that masquerades as rounded shoulders — the palms often face the outer thighs, with a subtle but distinct forward protrusion at the front of the joint that is not mirrored at the top of the shoulder. Two different postural pictures. Two very different problems. One simple observational screen that most people have never had done.
If you have been doing rows, face pulls, and band pull-aparts for months without meaningful improvement in shoulder pain or position, this distinction may be why.
Rounded Shoulders: What It Actually Means Anatomically
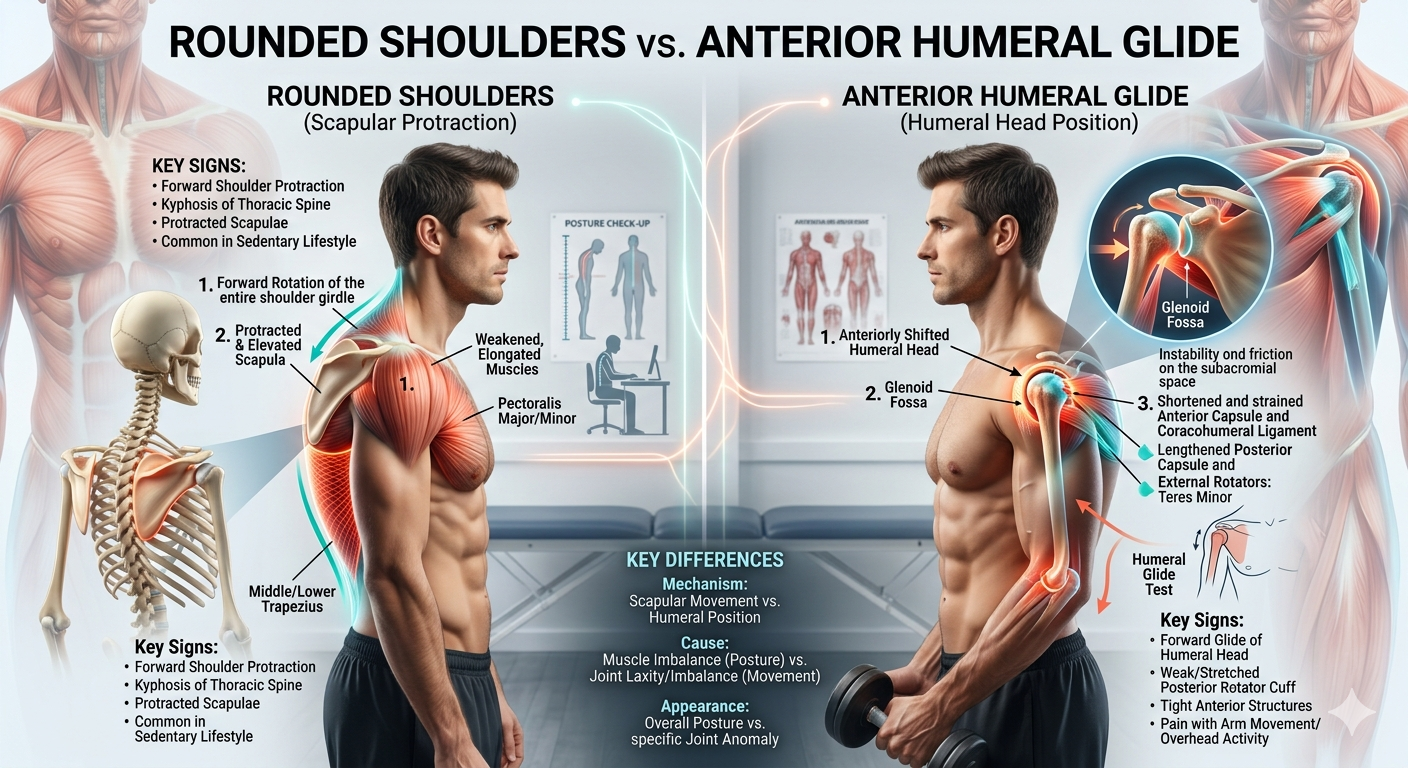
Rounded shoulders — the clinical term is scapular protraction — is a postural problem centered on the shoulder blade. The scapula migrates forward and outward, away from the spine, as a unit. When this happens, several things follow: the chest narrows and appears compressed, the upper back curves into kyphosis, the head translates forward, and the arms hang forward of the body’s midline.
The internal rotation of the arms in this position is what rotates the palms backward. When you look at someone with true rounded shoulders from behind, the shoulder blades are clearly winged away from the spine and often riding higher than they should. The entire shoulder complex — scapula, clavicle, and the proximal humerus — has shifted forward together.
The cause is almost always a combination of sustained poor posture, weak mid-trapezius and rhomboids, tight pectoralis major and minor, and often a stiff thoracic spine underneath all of it. The scapula is out of position, but the shoulder joint itself is structurally intact — the ball is still sitting reasonably well in the socket.
The standard correction for this pattern — scapular retraction exercises, rows, face pulls, anterior chest stretching — works when this is the actual diagnosis. The problem is that it does not work when the underlying problem is something else entirely.
Anterior Humeral Glide: The Problem Inside the Joint
Anterior humeral glide (AHG) is a different kind of problem — and it is subtle enough that it is frequently missed, labeled as rounded shoulders, and treated accordingly without success.
In AHG, the problem is not the position of the scapula. It is the position of the humeral head — the ball of the shoulder joint — within the glenoid socket. The humeral head has translated anteriorly: it has shifted forward within the joint capsule. Not a dislocation, not even close. We are talking about a few millimeters of anterior shift. But those millimeters alter the mechanics of every shoulder movement, compress the anterior joint capsule, and put the rotator cuff and bicipital tendon in a compromised position that generates pain with specific movements.
What causes this? The most common pattern I see is a combination of anterior capsule laxity (the front of the joint has become loose, often from repetitive forward movement patterns or hypermobility), relative tightness of the posterior capsule (the back of the joint), and weakness of the external rotators and posterior Rotator cuff. The subscapularis — the front-facing rotator cuff muscle — often contributes to the anterior pull when it becomes chronically shortened. The result is a humeral head that has crept forward in its socket, year by year, until it finally started generating symptoms.
How to Tell Them Apart
The visual and functional differences between rounded shoulders and AHG are real, though they require knowing what to look for.
Where the forward position appears. In rounded shoulders, the entire shoulder complex moves forward as a unit — you see the shoulder blade migration and the overall collapse of the upper back. In AHG, the front of the joint itself protrudes. There is often a visible fullness or forward prominence specifically at the anterior shoulder, just below the front of the collarbone, while the top of the shoulder may appear relatively normal. The blade position alone does not explain what you are seeing.
What the palms do at rest. This is the quick screen I mentioned at the start. True rounded shoulders rotate the arms into internal rotation — palms face backward. In AHG, the humerus may actually sit in relative external rotation, with the palms facing the outer thighs or even slightly forward. This is because the anterior capsule tightness pattern does not necessarily drive the same whole-arm internal rotation seen in scapular protraction.
The pain pattern with specific movements. Rounded shoulders typically generate pain with reaching overhead, behind the back, or across the body — impingement patterns from the scapular position affecting subacromial space. AHG tends to generate pain at the very front of the shoulder, often with bicep curl motions, chest press movements, or any loading of the shoulder in a forward-flexed position. Push-ups are frequently provocative. Overhead work is often fine or only mildly uncomfortable.
Response to scapular retraction. In rounded shoulders, retraction exercises provide noticeable relief by unloading the shoulder mechanism. In AHG, pulling the scapulae back without addressing the anterior humeral position often changes nothing — or occasionally makes anterior shoulder discomfort worse, because the scapular movement alone does not restore the ball to its correct position in the socket.
A Self-Assessment You Can Do Right Now
Stand in front of a mirror, profile view. Relax your arms completely. Observe: does the protrusion you see at the shoulder appear at the top of the shoulder and along the entire front of the chest? That is more consistent with the whole-complex forward shift of rounded shoulders. Does the protrusion appear specifically at the front of the joint itself, below the collarbone, while the upper shoulder appears relatively neutral? That is more consistent with AHG.
Now try this: gently draw your shoulder blade backward — not a hard retraction, just a gentle nudge. Does this noticeably change the position of the front of the joint, reducing that forward prominence? If yes, the scapular position is a significant driver, which aligns more with rounded shoulders. If the blade moves but the front of the joint still bulges forward unchanged, the humeral head position may be a more primary issue.
Finally, do a simple external rotation test. With your elbow bent to 90 degrees at your side, rotate your forearm outward away from your body. Note whether this feels restricted or tight — and whether it changes the feeling at the front of the shoulder. Restricted external rotation with anterior shoulder tightness during this movement is a clinical indicator of AHG I look for consistently in evaluations.
Why Treating the Wrong Pattern Makes Things Worse
This is where the clinical stakes are real. Scapular retraction exercises — rows, band pull-aparts, face pulls — done aggressively into a shoulder with anterior humeral glide can actually worsen the anterior capsule stress. The retraction motion compresses the anterior joint when the humeral head is already sitting forward; you are pulling the joint into a position that loads the already-compromised anterior structures.
Similarly, anterior chest stretching — doorway pec stretches, for example — in someone with AHG can stress the anterior capsule directly. The pectoralis minor is often involved in AHG, but aggressive anterior chest stretching without first addressing humeral head position can increase instability in a joint that already lacks anterior support.
The correct sequence for AHG begins with posterior capsule stretching and posterior chain activation — specifically the posterior rotator cuff and lower trapezius — to draw the humeral head back and create posterior balance. External rotation strengthening in neutral and in slight abduction (side-lying external rotation, sidelying ER at 90 degrees abduction) is foundational. Only after the humeral head position is restored does scapular positioning work become productive rather than counterproductive.
When to Get a Proper Evaluation
If your shoulder pain is significant, has been present for more than six to eight weeks despite consistent self-care, or is accompanied by any clicking, catching, or locking sensation within the joint — please have it evaluated in person. Anterior shoulder pain with specific movements can have several overlapping causes: bicipital tendinopathy, anterior labral tears, subscapularis involvement, and AC joint issues can all produce anterior shoulder discomfort that resembles the AHG pattern from the outside. Distinguishing these requires orthopedic testing that cannot be replicated with a mirror.
The good news for most people whose shoulder has been labeled “rounded” and treated accordingly without improvement: the problem is often not that the treatment was wrong in principle. It is that it was aimed at the wrong structure. Getting the right diagnosis changes the intervention, and for most AHG presentations, the right intervention produces meaningful change within four to six weeks.
— Calli, DC, LE | Licensed Chiropractor & Esthetician, Los Angeles
Medical disclaimer: This article is for educational purposes only and does not constitute a clinical diagnosis or treatment recommendation. Shoulder pain accompanied by weakness, instability, severe restriction of movement, or symptoms following a specific injury should be evaluated by a qualified healthcare provider.
Related: Shoulder Impingement Syndrome: Why Medical Treatment Alone Fails