By Calli | Licensed Chiropractor & Esthetician (DC, LE) | May 3, 2026
A bad headache is a bad headache. But the painkiller that calms one type can do almost nothing for another, and the lifestyle change that prevents one can be completely irrelevant to the other. After 20 years of treating headache patients in my Los Angeles clinic, the mistake I see most often is that people treat every headache the same way — popping the same tablet, blaming the same trigger, and never figuring out which kind they actually have. The result is years of headaches that never quite go away.
Tension headaches and migraines are the two most common headache types in adults. They feel different. They start differently. They respond to different treatment. And there is a third category most people have never heard of — cervicogenic headache, the kind your neck is producing — that I have watched get misdiagnosed as either of the other two for years before someone finally checks the upper cervical spine.
I am Calli, a licensed chiropractor in Los Angeles. Headaches are one of the most common reasons patients walk into my office. This is the same plain-language breakdown I give them on their first visit — how to tell tension, migraine, and neck-driven headaches apart, and what actually helps each one.
TABLE OF CONTENTS
Quick Summary
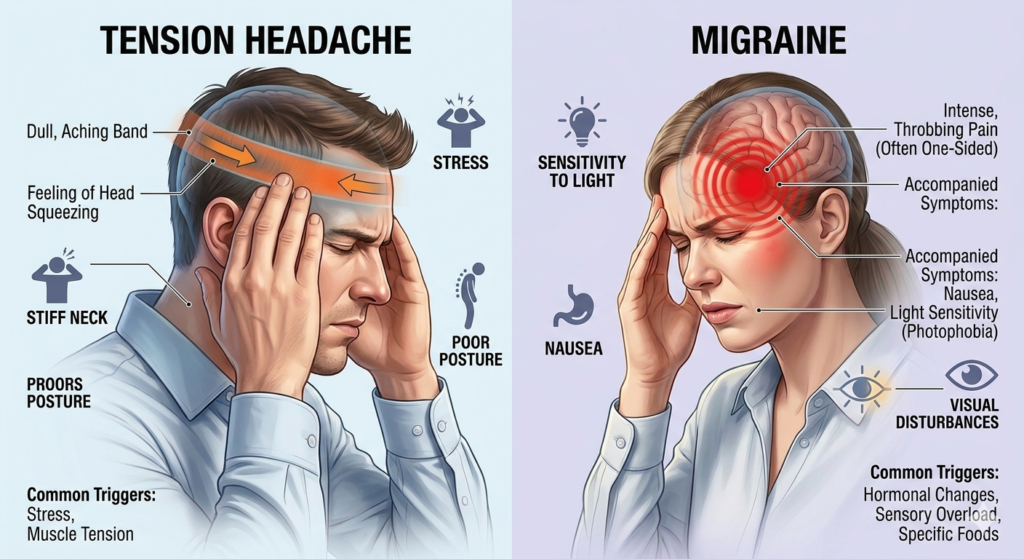
Tension headache: a steady, pressing, band-like pain on both sides of the head, mild to moderate in intensity, no nausea, no light sensitivity, often triggered by stress and posture. Migraine: a one-sided, throbbing, moderate-to-severe pain that worsens with movement, often with nausea, light sensitivity, and visual changes. Cervicogenic headache: pain that starts at the base of the skull or upper neck and radiates forward, often one-sided, often triggered by neck position. The treatment for each is meaningfully different — and getting the diagnosis right is the difference between three days of misery and twenty minutes of relief.
WHY TRUST CALLI
I am a licensed Doctor of Chiropractic and licensed Esthetician with 20 years of practice in Los Angeles. Headaches — particularly the neck-driven kind that get mislabeled as migraines — are part of my regular caseload, worked up using cervical motion palpation, suboccipital provocation testing, and a combination of upper cervical mobilization, Diversified technique, and instrument-assisted soft tissue mobilization (IASTM). This article is educational and is not a substitute for medical evaluation.
What Does a Tension Headache Actually Feel Like?
Tension-type headache is the most common headache in adults, and the most common headache I work up in my LA clinic. The hallmark: it feels like a tight band wrapping around your head, pressing in evenly from both sides. Not throbbing. Not stabbing. Just a steady, dull pressure that builds over hours.
Classic Tension Headache Symptoms
- Bilateral pressure — both sides of the head, not one
- Mild to moderate intensity — annoying, not disabling
- Steady ache rather than throbbing
- Often radiates from the back of the head and neck forward
- No nausea, usually no significant light or sound sensitivity
- Pain does not significantly worsen with normal physical activity
The tension headache patient I see most often in my LA practice is a 25–45-year-old desk worker who tells me the headache builds slowly through the afternoon and is gone by morning — but is back the next day.
Common Tension Headache Triggers
The biggest drivers in 2026 are surprisingly mechanical, and after 20 years they have not changed much — the technology has just made them worse: prolonged screen time, jaw clenching at night, sleep disruption, dehydration, caffeine withdrawal, and emotional stress. The reason “stress headache” became a household phrase is that the upper trapezius muscles tighten during stress, the suboccipital muscles at the base of the skull get pulled with them, and you end up with referred pain across the head. When I palpate the upper traps and suboccipitals on a tension headache patient, the pattern is almost always the same.
What Are the Real Symptoms of a Migraine?
Migraine is a neurological condition, not just a bad headache. Patients who have only ever had tension headaches sometimes call any severe headache a “migraine.” A real migraine has a specific symptom pattern that, once you know it, is hard to confuse with anything else — and the patients I refer back to a primary care physician or neurologist are the ones whose history fits this picture squarely.
Classic Migraine Symptoms
- Pain typically on one side of the head (though can be both)
- Throbbing or pulsating quality
- Moderate to severe intensity — often disabling
- Worsens with normal activity (climbing stairs, bending over)
- Nausea, sometimes vomiting
- Strong sensitivity to light, sound, or smells
- Lasts 4 to 72 hours if untreated
The Migraine Aura: A Telltale Sign
About a third of migraine patients experience an aura — a neurological warning before the pain begins. Auras can include zigzag visual lines, blind spots, tingling on one side of the face or hand, or temporary speech changes. In my LA caseload, when a patient describes an aura that lasts under an hour and resolves before or during the headache, I am thinking typical migraine. New neurological symptoms that do not resolve, or that affect one side of the body persistently, are not migraine — and I refer those out for immediate medical evaluation.
Common Migraine Triggers
Hormonal shifts, certain foods (aged cheese, red wine, processed meats, MSG), skipped meals, sleep deprivation or oversleeping, weather changes, and bright or flickering light. Many of the migraine patients I see in clinic have one or two specific triggers they can identify with a headache diary, and avoiding those triggers cuts attack frequency dramatically. The headache diary is one of the very first homework assignments I give a suspected migraine patient.
The Headache Most People Miss: Cervicogenic (Neck) Headache
This is the headache that gets diagnosed as a migraine for years before someone finally looks at the neck. Cervicogenic headache literally means “headache coming from the cervical spine” — the neck. After 20 years in Los Angeles, this is the headache type I have seen explode in frequency, and the reason is simple: the average patient I treat now spends six to ten hours a day looking down at a screen.
How to Recognize a Cervicogenic Headache
- Pain starts at the base of the skull or upper neck and travels forward
- Almost always one-sided — same side, attack after attack
- Triggered or worsened by neck movement or sustained head positions
- Tenderness when pressing into the upper neck on the affected side
- Usually no aura, no severe nausea, no light sensitivity
- Pain often described as a deep, dull, “behind the eye” ache
The patient pattern I see most often: a 28–50-year-old who works on a laptop or phone for most of the day, whose headaches come from the same side every time, and who has been told for years that they have migraines.
Why Sitting and Screens Are Driving This Headache Up
When your head sits forward of your shoulders for hours, the small joints at the top of the cervical spine get compressed, and the muscles at the base of the skull go into protective spasm. Those muscles share nerve pathways with the trigeminal nerve, which supplies the face and front of the head. The brain literally cannot tell the difference between a signal from your neck and a signal from your forehead — so neck pain is felt as headache. The same prolonged screen-and-sitting pattern that destroys lower backs is now driving a generation of headaches I see in clinic. I covered the spine side of this in why sitting all day destroys your spine.
How to Tell Tension Headache From Migraine in Under a Minute
The fastest way to triage your own headache is to run through five quick questions — the same five I run through during the first minute of an intake. The pattern of yes/no answers usually points clearly to one of the three.
The 5-Question Headache Triage
1. Is the pain on one side or both sides? Both → tension. One side → migraine or cervicogenic.
2. Is the pain throbbing or pressing? Throbbing → migraine. Pressing → tension or cervicogenic.
3. Do you feel nauseated or sensitive to light? Yes → migraine. No → tension or cervicogenic.
4. Does normal activity make the pain worse? Yes → migraine. No (or only neck movement does) → tension or cervicogenic.
5. Does it start at the base of your skull and move forward? Yes → cervicogenic. No → tension or migraine.
When a Headache Is a Medical Emergency
Stop self-diagnosing and seek immediate medical evaluation if you experience: the worst headache of your life with sudden onset (sometimes called a “thunderclap” headache), a headache with fever and stiff neck, a headache with confusion or weakness on one side of the body, a headache after a head injury, or a new headache pattern in someone over 50. These can be signs of conditions that need urgent care. In 20 years of clinic, the small number of patients I have flagged with these red flags I have referred out to the ER on the spot — this is the one situation where conservative care has no place.
What Actually Helps Each Type of Headache
The right intervention depends entirely on the type. Generic “headache hacks” are why patients stay stuck in the cycle — that pattern is one I have to break with new patients every week.
What Helps a Tension Headache
Hydration, a meal if you skipped one, gentle neck and shoulder stretching, stepping away from a screen, and over-the-counter pain relievers like acetaminophen or ibuprofen used appropriately. The most underused intervention I prescribe to my LA patients: a 10-minute walk outside. Movement relaxes the cervical and trapezius muscles, and natural light helps reset the autonomic nervous system. In my clinical experience, many tension headaches are gone within 30 minutes of that walk.
What Helps a Migraine
Migraine treatment falls into two categories. Acute treatment (during the attack): triptan medications prescribed by your doctor, lying in a dark quiet room, ice on the head or neck, hydration, and avoiding food triggers. Preventive treatment (between attacks): identifying triggers via a headache diary, magnesium and riboflavin supplementation (often suggested by neurologists), regular sleep and meals, and prescription preventives if attacks are frequent. Migraine is a medical condition that benefits from a relationship with a primary care physician or neurologist, and my role with these patients is usually to address any cervical contribution alongside their medical management.
What Helps a Cervicogenic Headache
This is the headache type that responds best to manual care, and it is where the bulk of my own headache work happens. In my LA office, the protocol I run on cervicogenic headache patients is a combination of upper cervical mobilization, suboccipital release, deep neck flexor strengthening, IASTM along the upper trapezius, and posture correction over weeks. Generic neck stretches help temporarily; structured care from a chiropractor or physical therapist using techniques like Diversified, Activator, or Cox cervical distraction usually resolves the pattern. Sleep position matters too — if you wake up with headaches, your pillow height and sleep posture are part of the chain. I cover the sleep side of this in the best sleeping position for back pain.
When to Seek Professional Care for Headaches
If headaches occur more than twice a week, last more than four hours regularly, are not responding to over-the-counter treatment, are interfering with work or sleep, or have changed in character recently — my clinical recommendation is to get evaluated. A primary care physician for medical workup. A chiropractor or physical therapist if the pattern points cervicogenic. A neurologist if migraines are frequent or severe. Headaches are not a diagnosis — they are a symptom. The job is to find what is driving them.
The Bottom Line
Tension headaches feel like a band squeezing both sides of your head. Migraines feel like a throb on one side, with nausea or light sensitivity. Cervicogenic headaches start at the base of the skull and march forward — and they are the kind I see most often misdiagnosed in 2026 because so much of life is spent looking down at a screen. The treatment for each is genuinely different. Identify which one you are having, treat it appropriately, and get professional evaluation if headaches are frequent, severe, sudden, or changing in character.
Calli’s Clinical Note
In 20 years of running an LA practice, the easiest test for cervicogenic headache is one I do at the very start of every headache exam. I press into the upper neck on the side where the patient feels their headaches. If pressure on a specific spot reproduces or intensifies the same head pain they have been experiencing, the headache is at least partly coming from the neck. That single finding shifts the treatment plan immediately — from drug management to manual care with techniques like upper cervical mobilization and IASTM. If you have been treating “migraines” for years with limited success and your headaches always start at the base of the skull on the same side, please get a clinical exam from someone who knows how to assess the upper cervical spine. The relief that comes from finally addressing the right driver — after years of treating the wrong one — is one of the most satisfying parts of my work.
Related Reading
Why Does Your Hip Pinch When You Sit? →
If sitting reproduces a sharp pinch in the front of your hip, that is not a tight muscle. The next post explains the hip impingement pattern that is showing up in younger and younger patients — and how to tell whether what you have actually needs surgery.
— Calli
DC, LE | Licensed Chiropractor & Esthetician | The right diagnosis is the shortest path to relief.
Medical disclaimer: This article is for educational purposes only and is not a substitute for evaluation by a qualified healthcare provider. Sudden, severe, or unusual headaches — especially those accompanied by fever, vision loss, weakness, confusion, or stiff neck — require immediate medical evaluation.