By Calli | Licensed Chiropractor & Esthetician (DC, LE) | May 3, 2026
Your MRI report says “disc bulge at L4-L5.” Your friend’s report says “herniated disc at L5-S1.” You both have low back pain. You both feel terrified you’ll need surgery. And neither of you actually knows what those words mean — because the radiologist wrote them in three lines and walked away.
Here is what almost no one explains: a bulging disc and a herniated disc are not two different diseases. They are two points on the same timeline. One is the early warning. The other is the one that finally pinches a nerve. After 20 years of reading disc imaging in my Los Angeles clinic, I can tell you that most patients who panic over an MRI report do not actually need surgery, and most patients who ignore early disc warning signs end up with the version that does.
I am Calli, a licensed chiropractor in Los Angeles, and disc cases are part of my caseload every single week. This is the exact explanation I give my own patients on their first visit — what each one actually is, how to tell them apart from your symptoms (not just your MRI), and what real recovery looks like in 2026.
TABLE OF CONTENTS
Quick Summary
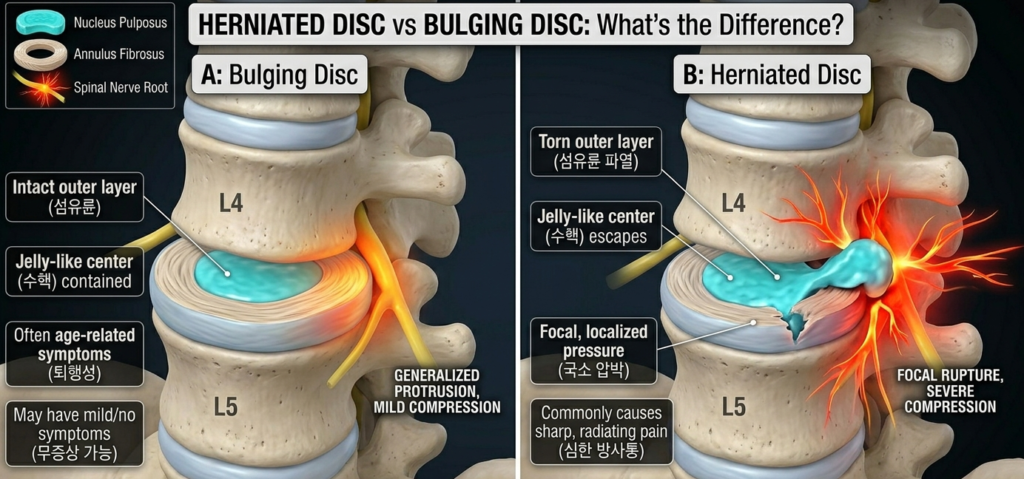
A bulging disc means the outer ring of a disc has weakened and is pushing outward — but the inner gel is still inside. A herniated disc means that outer ring has actually torn, and the inner gel has leaked out. A bulge is a warning. A herniation is a rupture. Most bulges and even most herniations heal without surgery if you stop the movement patterns that caused them and let the disc reabsorb fluid over 6–12 weeks.
WHY TRUST CALLI
I am a licensed Doctor of Chiropractic and licensed Esthetician with 20 years of practice in Los Angeles. Disc cases are part of my daily caseload, and I work them up using a combination of orthopedic exam, McKenzie centralization assessment, and Cox flexion-distraction protocols. This article is educational and not a substitute for a clinical exam — but it is the same plain-language breakdown I give in office.
What Is a Spinal Disc and How Does It Get Damaged?
Before we compare a bulge to a herniation, you need to know what a disc actually is. Between every two vertebrae in your spine sits a small cushion. That cushion has two parts: a tough outer ring made of crisscrossed cartilage fibers (called the annulus fibrosus), and a soft inner gel center (called the nucleus pulposus). The outer ring keeps the gel locked inside. The gel absorbs shock when you walk, sit, lift, twist, sneeze, or simply stand against gravity all day.
Why Discs Wear Down: The 3 Real Causes of Disc Damage
In my 20 years of practice in Los Angeles, I have learned that discs do not get damaged by one bad lift. They get damaged by a thousand small ones. The three patterns I see most often in my exam room:
1. Sustained sitting with a rounded lower back. When you slouch forward, the front of the disc gets compressed and the gel migrates backward — toward the spinal nerves. Eight hours a day of that, five days a week, slowly weakens the back wall of the disc. The patient I see most often for a fresh disc bulge is a 30–50-year-old desk worker whose flare started after a long flight, a long drive, or a stretch of unusually intense workdays. I covered the upstream mechanic in why sitting all day is destroying your spine.
2. Lifting with a rounded back. Same mechanic, much higher load. Picking up a laundry basket, a child, or a grocery bag with your back rounded delivers a focal load right where the disc is already thinning. When I take a history and the patient says “it started right after I helped a friend move,” I am almost always looking at a fresh disc injury.
3. Dehydration and age. Discs are 80% water in your twenties. By your forties, they have lost meaningful hydration. A drier disc is a more brittle disc. This is why the same movement that did nothing at 25 produces a bulge at 45 — a pattern I have seen reliably in my LA caseload across two decades.
Bulging Disc vs Herniated Disc: The Real Anatomical Difference
Here is the simplest accurate way to think about it, and the analogy I use with my patients in the exam room:
A bulging disc is when the outer ring is still intact, but it has weakened and bulges outward — like a tire that is over-inflated and pushing out a soft spot on its sidewall. The gel inside is still contained.
A herniated disc is when that sidewall has actually torn, and the gel inside has leaked out into the space where your spinal nerves live. Older terms you may hear for the same thing: ruptured disc, slipped disc, prolapsed disc, extruded disc. They all refer to the same anatomy.
Is a Bulging Disc Less Serious Than a Herniated Disc?
In general, yes — but not always, and this is one of the most common misunderstandings I correct in clinic. The reason is that what causes the pain is not the disc itself. It is whether the bulged or herniated material is touching a nerve. In my exam room I have seen small herniations that pointed away from the nerve root and were completely silent, and large bulges that pressed directly on a nerve and produced disabling symptoms. So the label matters less than the location, and the symptoms in front of me matter more than either.
What Does a Bulging or Herniated Disc Look Like on an MRI Report?
Common phrases on a real MRI report — I read several of these every week:
- “Disc desiccation” — the disc has lost water. Normal aging finding, often present without symptoms.
- “Diffuse disc bulge” — the whole back wall is pushed outward evenly. Usually mechanical, usually responds to conservative care.
- “Focal disc protrusion” — one spot is pushing outward. Closer to a herniation.
- “Disc extrusion” — the gel has come out of the disc capsule. This is a true herniation.
- “Sequestration” — a fragment of disc material has broken off completely. The most serious form, occasionally needs surgery.
Bulging Disc Symptoms vs Herniated Disc Symptoms (Side-by-Side)
Imaging will eventually tell you the structural answer. But your body will tell you the functional answer first. Here is how the two typically present in the patients I see at my LA clinic.
Common Bulging Disc Symptoms
- Dull, achy lower back pain that comes and goes
- Pain that worsens with prolonged sitting or driving
- Stiffness in the morning that loosens up after walking
- Mild radiation into the buttock, but rarely past the knee
- No major weakness, no foot drop, no numbness in the toes
The bulging disc patient I see most often is the 35–50-year-old who comes in saying “I’ve had on-and-off back stiffness for two years and now it’s getting worse.” That low-grade timeline is the bulge talking.
Common Herniated Disc Symptoms
- Sharp, electric, or burning pain that travels from the lower back down the leg past the knee (this is true sciatica — see what actually causes sciatica)
- Pain that worsens dramatically with coughing, sneezing, or straining
- Numbness or tingling in a specific patch of the leg or foot
- Weakness when raising the big toe, or weakness pushing off the floor
- Pain so severe that lying flat is the only relief
When I run the straight leg raise test in my office and lifting the affected leg to 30–45 degrees reproduces sharp pain down the calf, that is one of the most reliable in-clinic confirmations of disc herniation I have.
When Disc Symptoms Become a Medical Emergency
The one disc presentation that is a true emergency is called cauda equina syndrome. It is rare, but every chiropractor I trained with drilled this list because it cannot wait. Signs: numbness in the inner thighs, groin, or saddle area; new loss of bladder or bowel control; severe weakness in both legs at once. If you have any of these, do not finish reading this article. Go to an emergency room. This is the single situation where surgical decompression is truly time-critical, and in 20 years I have referred a small number of patients out emergently for exactly this.
Which Disc Problems Actually Need Surgery in 2026?
This is the part patients are most afraid of, and it is also the part where the data has changed the most in the last decade. It is also where I spend the most reassurance time on a first visit.
The current evidence supported by spine surgery research is that the majority of disc bulges and even disc herniations resolve on their own over 6 to 12 weeks. The body actually reabsorbs the leaked gel through natural inflammatory processes. Imaging studies have repeatedly shown that herniations visible on the first MRI are smaller or gone entirely on the follow-up MRI taken months later — without any surgery in between. I have watched this play out with my own LA patients hundreds of times.
When Disc Surgery Is Actually Recommended
A spine surgeon will typically recommend surgery only when one of the following is true: cauda equina syndrome (above), progressive neurological loss (worsening weakness or numbness despite conservative care), or pain that has not improved after 6 to 12 weeks of structured non-surgical treatment. If none of those three conditions apply, conservative care is the standard first line. In my own practice, the percentage of disc patients I have ever needed to refer out for surgical consult has stayed under five percent across two decades.
What “Conservative Care” Actually Means
It is not just rest. Bed rest beyond two days actually slows recovery — that is one of the strongest pieces of evidence we have. Modern conservative care for disc problems means: targeted spinal manipulation or mobilization, specific decompression-style exercises (the McKenzie method is the most studied), modified daily movement, anti-inflammatory support, and a return-to-activity plan. In my Los Angeles office I run most acute disc cases on a combination of Cox flexion-distraction (a gentle decompressive technique on a specialized table) and a graded McKenzie press-up program. Done correctly, this resolves most cases.
How to Heal a Disc Bulge or Herniation Without Making It Worse
If your imaging shows a bulge or herniation and your symptoms are not in the emergency category above, this is the playbook I give my own patients on their first visit.
Stop the Three Movements That Push the Disc Backward
Anything that loads your spine in flexion (forward bending) pushes the gel further into the back wall. The three biggest culprits I see in my LA clinic during a flare: sitting in a slouched chair for hours, lifting anything from the floor with a rounded back, and toe-touch stretches. Toe touches feel like they should help — they don’t. I have had to talk countless yoga regulars out of them. They actively worsen most disc cases.
Use Extension to Move the Disc Forward
The McKenzie press-up is the most evidence-supported home movement for disc-related pain, and it is the first home exercise I assign in my Los Angeles practice. Lie face down on the floor. Place your hands flat under your shoulders. Slowly press your upper body up while keeping your hips on the floor. Hold 2 seconds. Lower. Repeat 10 times. Do this every 2 hours during the acute phase. For most centralized disc pain, my clinical observation is that this single movement is the most effective thing you can do at home.
Walk, Don’t Rest
Walking on flat ground for 10 to 20 minutes, several times a day, pumps fluid through the disc and supports healing. Lying in bed for days does the opposite. Move gently and often — this is the single piece of advice I have to repeat most often to LA patients who came in expecting to be told to rest.
Reset Your Hip and Pelvis Mechanics
Many disc cases are downstream of hip stiffness. When the hip cannot extend properly, the lower back compensates with extra motion and load on the disc. In 20 years, I have lost count of how many disc patients were genuinely surprised that fixing their hip mechanics is what finally let their lumbar disc settle. I cover the hip side of this in why your hip pinches when you sit.
When to See a Chiropractor or Physical Therapist
If self-care has not made meaningful improvement in two weeks, get hands-on care. A trained chiropractor or physical therapist can confirm the location of the disc problem with a clinical exam, identify which side and direction the gel has shifted using something like the McKenzie repeated-movement assessment, and guide you through the specific exercises and adjustments your case actually needs. Generic advice plateaus quickly. A skilled clinician using techniques like Cox flexion-distraction, IASTM, or Diversified mobilization will not.
The Bottom Line
A bulging disc is a warning. A herniated disc is the rupture that warning was pointing to. Most cases of both heal on their own within 6 to 12 weeks if you stop loading your spine in forward flexion, restore extension with daily press-ups, walk often, and address the hip mechanics that were overloading the disc in the first place. Surgery is reserved for the small subset with worsening neurological loss or cauda equina symptoms. Imaging is useful, but your symptoms — not the words on the MRI report — drive your treatment plan.
Calli’s Clinical Note
In 20 years of running an LA practice, the single most predictive question I ask is not “where does it hurt” — it is “what makes it better.” If the answer is “lying down with my legs up” or “leaning back,” the disc is involved. If the answer is “leaning forward over a shopping cart” or “sitting curled up,” I am thinking stenosis, not disc. The same imaging finding can mean very different things depending on which position relieves you. That is why a clinical exam — with hands-on tests like McKenzie centralization, the slump test, and Cox flexion-distraction trial — still matters more than an MRI report alone.
Related Reading
What Causes Sciatica Pain? A Chiropractor Explains the Real Source (and How to Fix It) →
What Is Spinal Stenosis? Symptoms, Causes, and What Actually Helps →
If your pain gets worse standing and better sitting, your problem is probably not a disc. The next post breaks down the spinal narrowing condition that mimics disc pain — and the very different treatment approach it requires.
— Calli
DC, LE | Licensed Chiropractor & Esthetician | Real diagnosis comes from your story, not just your scan.
Medical disclaimer: This article is for educational purposes only and is not a substitute for evaluation by a qualified healthcare provider. New or worsening neurological symptoms — including loss of bladder or bowel control, saddle numbness, or progressive leg weakness — require urgent medical evaluation.