By Calli | Licensed Chiropractor & Esthetician (DC, LE) | May 3, 2026
You can walk to the mailbox, but not to the end of the block. You feel fine pushing a shopping cart, but the moment you stand still in line, your legs start to ache and burn. You bend forward and the pain disappears almost instantly. Your friends keep telling you it sounds like sciatica. It is not sciatica. It is something else, and the treatment looks almost completely different.
The condition you are describing has a name: lumbar spinal stenosis. After 20 years of practice in Los Angeles, I can tell you it is one of the most common reasons patients over 50 stop walking for exercise — and one of the most under-recognized causes of leg pain I see in my exam room. The good news: it is also one of the most responsive to the right kind of conservative care, even though most patients I meet have been told their only option is surgery.
I am Calli, a licensed chiropractor in Los Angeles. This article is the same plain-language explanation I give my patients during their first visit — what spinal stenosis actually is, the symptoms people miss, why it tricks doctors into thinking it is sciatica, and the treatment approach that actually moves the needle in 2026.
TABLE OF CONTENTS
Quick Summary
Spinal stenosis is a narrowing of the canal that holds your spinal cord and nerves. The classic sign: your legs feel heavy, burning, or weak when you walk or stand, but the symptoms vanish almost immediately when you sit down or bend forward over a counter. It is the opposite of a herniated disc, which usually feels worse when you sit. Treatment focuses on flexion-based exercise, hip mobility, walking with a temporary forward lean, and decompressive techniques — surgery is a last resort, not a first one.
WHY TRUST CALLI
I am a licensed Doctor of Chiropractic and licensed Esthetician with 20 years of practice in Los Angeles. Stenosis cases — especially in patients over 50 — are part of my regular caseload, worked up using flexion-based assessment, hip mobility testing, and a combination of Cox flexion-distraction and Diversified mobilization. This article is educational and is not a substitute for a clinical exam.
What Is Spinal Stenosis in Plain English?
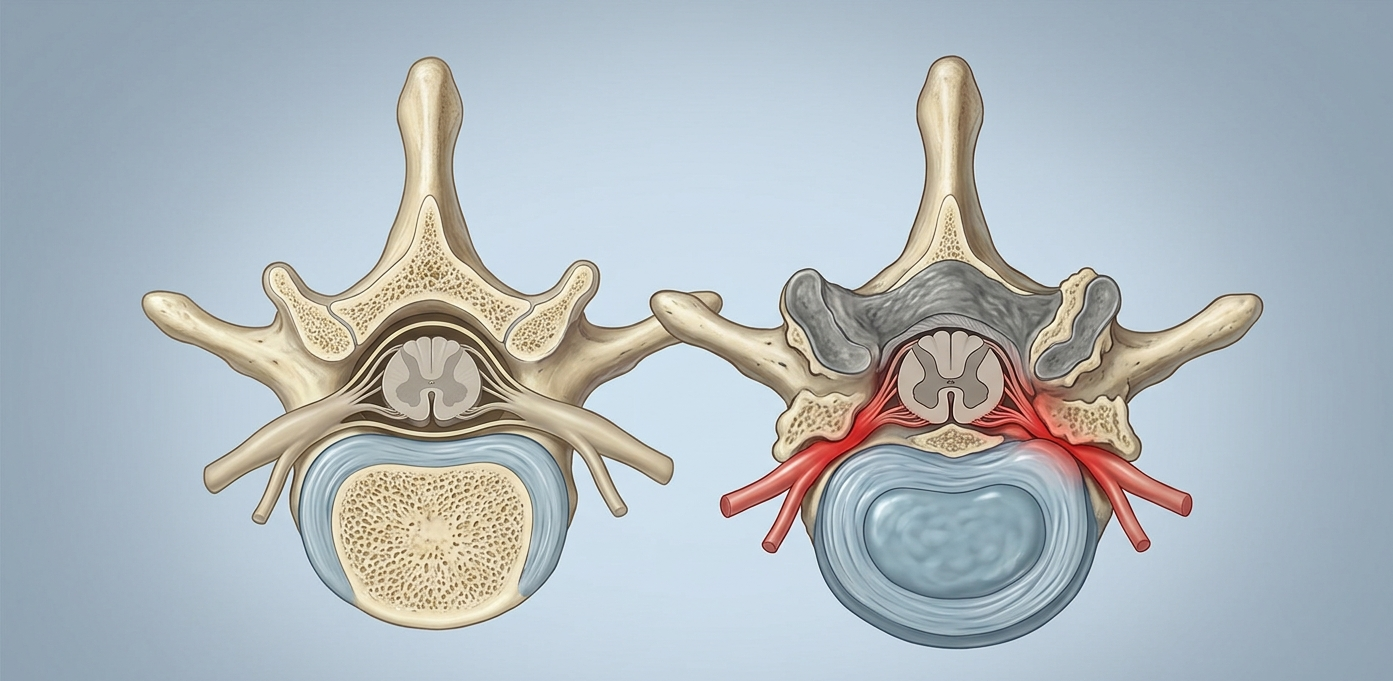
Picture your spinal cord as an electrical cable running through a bony tunnel from the base of your skull down to your tailbone. That tunnel is called the spinal canal. Stenosis simply means the tunnel has narrowed. When it narrows enough to start crowding the nerves running through it, you start to feel it — usually in your legs, sometimes in your buttocks, and occasionally in both at once.
In my LA practice, the stenosis patient I see most often is a 55–75-year-old who tells me “I used to walk two miles every morning and now I can barely make it to the mailbox without my legs giving out.” That timeline — gradual reduction in walking distance over months or years — is the single clearest history pointer toward stenosis I have.
The Two Main Types: Central vs Foraminal Stenosis
Central canal stenosis is when the main tunnel itself narrows. This is what produces the classic “I cannot stand for long” symptoms.
Foraminal stenosis is when the small side openings where individual nerves exit the spine narrow. This produces more localized leg pain in the path of one specific nerve, and can mimic sciatica.
Many of my patients have a mix of both, which is part of why the same diagnosis label can produce slightly different presentations from one exam room to the next.
Where Spinal Stenosis Happens Most Often
The lower back (lumbar stenosis) is by far the most common location, and it is what I assess weekly in clinic. The neck (cervical stenosis) is the second most common. Lumbar stenosis affects the legs. Cervical stenosis can affect the hands, balance, and walking gait. This article focuses on lumbar stenosis — the type that drives the “my legs give out when I walk” pattern I hear so often during intake.
Spinal Stenosis Symptoms Most People Miss
The hallmark of stenosis is that the pain is positional. It is not constant. It comes on with one set of positions and disappears with another. In my 20 years of treating this condition, recognizing this pattern is what separates stenosis from almost every other low back condition I work with.
The Classic Stenosis Pattern: Worse Standing, Better Sitting
If your symptoms get worse the longer you stand or walk, and meaningfully better the moment you sit down or bend forward, that is stenosis until proven otherwise. The medical name for this is neurogenic claudication. The forward bend opens up the spinal canal slightly, taking pressure off the nerves. That is also why the patients I see with stenosis often unconsciously lean on a shopping cart, walker, or kitchen counter — and feel relief without realizing why. I can frequently spot this pattern within the first 60 seconds of watching a patient walk down my hallway, before any test has been done.
Other Common Spinal Stenosis Symptoms
- Heaviness, burning, or aching in one or both legs after walking a short distance
- The need to stop, sit, or lean forward to keep going
- Tingling or numbness in the calves, feet, or buttocks
- A feeling that your legs are “not yours” or might give out
- Symptoms that improve dramatically when riding a bike or pushing a cart
- Lower back stiffness on standing up from a chair
When I take a stenosis history, “I am fine when I push a shopping cart” is one of the highest-yield answers I get — and patients almost never volunteer it on their own because they did not realize it mattered.
Symptoms That Are Not Typical of Stenosis
Sharp, electric, shooting pain that travels in a single line down the leg with sneezing or coughing is more typical of a disc herniation, and when I run the straight leg raise test on these patients it usually lights up the leg pain immediately. A deep groin pinch when sitting that disappears when you stand is more typical of a hip impingement, which I confirm in clinic with the FADIR test. Stenosis is the slow, building, position-dependent leg fatigue that you can almost set a timer to — and that is the version I see day after day in my LA exam room.
What Causes Spinal Stenosis to Develop?
Stenosis is overwhelmingly an age-related condition. The narrowing develops gradually, over years or decades, as several structures around the spinal canal slowly change. In my LA practice, the trajectory I see most often is that the patient had on-and-off low back episodes in their forties and fifties, and the stenosis itself only became symptomatic in their late fifties to seventies.
The Three Main Drivers of Spinal Narrowing
1. Disc height loss. As discs lose hydration and thin out with age, the bones above and below them sit closer together. The side openings where nerves exit get smaller.
2. Bone spurs (osteophytes). The body responds to long-term joint stress by laying down extra bone. Over years, these spurs encroach on the spinal canal. I see these reliably on the imaging of patients who first noticed stenosis symptoms in their sixties.
3. Ligament thickening. A ligament called the ligamentum flavum runs along the back of the spinal canal. With age and chronic loading, it thickens and bulges inward, narrowing the canal further.
Risk Factors That Speed It Up
Genetics play a role. Some patients are simply born with a smaller spinal canal — they may not develop symptoms until those age-related changes layer on top, and I have seen this stack of factors hit patients in their early fifties rather than their seventies. Other accelerators: long-term sedentary posture, repetitive heavy lifting, untreated spondylolisthesis, prior spinal surgery, and the same compounded sitting load I described in why sitting all day destroys your spine.
How to Tell Spinal Stenosis From Sciatica or a Herniated Disc
This is the single most important distinction to get right, because the treatment for stenosis and the treatment for a herniated disc move in nearly opposite directions. In my LA office, the most common reason a patient has been frustrated with prior care is that someone treated them for the wrong one.
The Position Test: Stenosis vs Disc
This is the same test I run during a new-patient consult. Sit down for ten minutes. Then stand up and walk for ten minutes. Notice which position made the leg symptoms worse.
- Worse with sitting, better with walking → think disc (see herniated disc vs bulging disc).
- Worse with standing or walking, better with sitting or bending forward → think stenosis.
- Sharp electric pain shooting down one leg past the knee with sneezing → think true sciatica from a disc (covered in what causes sciatica pain).
Why This Distinction Changes Your Treatment
For a herniated disc, my clinical recommendation is the McKenzie press-up — a back extension. For stenosis, that same press-up can make symptoms worse, because extending the spine further narrows the canal. Stenosis does better with flexion-based exercises: knees-to-chest, seated forward folds, stationary bike. Same body part, opposite movement. This is why a generic “back pain stretch” video on the internet is a coin flip — and why the patients who follow specific, exam-based prescriptions out of my office consistently outperform the patients who self-prescribe from social media.
Spinal Stenosis Treatment: What Actually Works in 2026
Despite what you may have been told, the first-line treatment for spinal stenosis is not surgery. The current evidence supports a structured conservative care plan as the starting point for nearly all stenosis cases that are not associated with progressive neurological loss — and over 20 years I have watched countless LA patients regain meaningful walking distance without ever stepping into a surgeon’s office.
Flexion-Based Exercise: The Foundation of Stenosis Care
Three movements I prescribe most often to my stenosis patients:
Knees-to-chest stretch. Lie on your back. Pull both knees gently toward your chest. Hold 20 seconds. Repeat 3 times. This opens the canal and gives nerves room.
Seated forward fold. Sit on the front edge of a chair. Bend forward, letting your hands rest near your ankles. Hold 30 seconds.
Stationary bike. Better than walking for cardiovascular fitness during a stenosis flare. The forward lean opens the canal while you exercise. This is the cardio prescription I give almost every stenosis patient who used to walk for exercise — it lets them keep their fitness without flaring symptoms.
The Walking Workaround: Use a Cart, Not a Cane
Many of my stenosis patients can walk much further leaning slightly forward over a shopping cart or grocery basket than they can walking upright. This is not a permanent solution, but during a flare it lets them keep moving without flaring symptoms further. Cardiovascular fitness during stenosis flares is critical — in my clinical experience, losing it makes everything worse, including the speed of recovery.
Hip Mobility Is the Hidden Lever
Tight hip flexors pull the lower back into more extension all day, which keeps the canal partially closed. Restoring hip extension is one of the most underused interventions in stenosis care, and it is one I emphasize on almost every stenosis patient I see. Daily kneeling hip flexor stretches and walking-based hip drills can meaningfully change the picture over 4 to 6 weeks. The hip pattern I see most often is the same one I describe in why your hip pinches when you sit.
When to Consider Injections or Surgery
Epidural steroid injections can offer a window of relief that lets you exercise productively. They do not cure stenosis, but they can break a pain-fear cycle that is preventing you from moving. Surgery — usually a decompressive laminectomy — becomes a real consideration only when conservative care has been tried for at least three months without improvement, when neurological symptoms are progressing, or when walking distance has dropped below the threshold required for daily life. In 20 years I have referred only a fraction of my stenosis patients out for surgical consult, and almost always after conservative care had been honestly tried.
The Bottom Line
Spinal stenosis is a narrowing of the canal that houses your spinal nerves, almost always caused by gradual age-related changes. Its hallmark is leg symptoms that worsen with standing or walking and improve with sitting or bending forward. Treatment in 2026 starts with flexion-based exercise, hip mobility, decompressive care, and structured walking workarounds — not surgery. Most cases improve significantly with the right program, and surgery is reserved for the smaller subset where conservative care has been honestly tried and the limits of daily life are being crossed.
Calli’s Clinical Note
In 20 years of running an LA practice, the most diagnostic moment with a suspected stenosis patient is asking them to walk down the hallway with me. Within thirty seconds, I can usually see the unconscious forward lean, the slight slowing, the small involuntary stop to “fix something on a shelf” that is really an excuse to bend forward and reset. That postural pattern — visible to anyone watching closely — tells me more than the MRI report sitting on my desk. If you recognize yourself in this article and your symptoms are positional, find a chiropractor or physical therapist who treats stenosis specifically and who uses techniques like Cox flexion-distraction and graded flexion-based loading. Generic back-pain advice is the wrong starting point for this condition.
Related Reading
What’s the Best Sleeping Position for Back Pain? →
If you wake up with more pain than you went to bed with, your sleep position is part of the problem. The next post breaks down the right and wrong positions for disc, stenosis, and sciatica — and the simple pillow strategy that fixes most of them.
— Calli
DC, LE | Licensed Chiropractor & Esthetician | The position that relieves your pain is the position your spine is asking for.
Medical disclaimer: This article is for educational purposes only and is not a substitute for evaluation by a qualified healthcare provider. New or worsening neurological symptoms — including loss of bladder or bowel control, saddle numbness, or progressive leg weakness — require urgent medical evaluation.